Pulmonary Tuberculosis
X-ray, Tuberculosis is an infectious disease that causes inflammation, the formation of tubercules and other growths within tissue, and can cause tissue death.
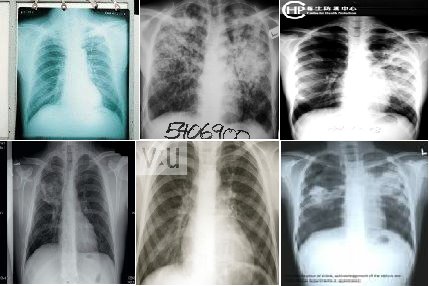
 These chest X-rays show advanced pulmonary tuberculosis. There are multiple light areas (opacities) of varying size that run together (coalesce).
These chest X-rays show advanced pulmonary tuberculosis. There are multiple light areas (opacities) of varying size that run together (coalesce).
Arrows indicate the location of cavities within these light areas. The X-ray on the left clearly shows that the opacities are located in the upper area of the lungs toward the back. The appearance is typical for chronic pulmonary tuberculosis but may also occur with chronic pulmonary histiocytosis and chronic pulmonary coccidioidomycosis. Pulmonary tuberculosis is making a comeback with new resistant strains that are difficult to treat. Pulmonary tuberculosis is the most common form of the disease, but other organs can be infected.
Another X-ray on this bellow shows a single lesion (pulmonary nodule) in the upper right lung (seen as a light area on the left side of the picture). The nodule has distinct borders (well-defined) and is uniform in density. Tuberculosis (TB) and other diseases can cause this type of lesion.

Typical signs of tuberculosis are:
- chronic or persistent cough and sputum production. If the disease is at an advanced stage the sputum will contain blood.
- fatigue.
- lack of appetite.
- weight loss.
- fever.
- night sweats.
Tuberculosis can mimic many forms of disease and must always be considered if no firm diagnosis has been made.
Other non-tuberculous mycobacteria found in soil and water can cause disease in susceptible patients with a history of cystic fibrosis, chronic lung damage, alcoholism and immunosuppression (suppression of immune responses by a disease or drugs). These atypical mycobacteria can be present as colonising organisms without necessarily causing disease.
Tuberculosis Treatment
Because administration of a single drug often leads to the development of a bacterial population resistant to that drug, effective regimens for the treatment of TB must contain multiple drugs to which the organisms are susceptible. When two or more drugs are used simultaneously, each helps prevent the emergence of tubercle bacilli resistant to the others. However, when the in vitro susceptibility of a patient's isolate is not known, which is generally the case at the beginning of therapy, selecting two agents to which the patient's isolate is likely to be susceptible can be difficult, and improper selection of drugs may subsequently result in the development of additional drug-resistant organisms.
Hence, tuberculosis is usually treated with four different antimicrobial agents The course of drug therapy usually lasts from 6-9 months. The most commonly used drugs are rifampin (RIF) isoniazid (INH), pyrazinamide (PZA ) and ethambutol (EMB) or streptomycin (SM). When adherence with the regimen is assured, this four-drug regimen is highly effective . Based on the prevalence and characteristics of drug-resistant organisms, at least 95% of patients will receive an adequate regimen (at least two drugs to which their organisms are susceptible) if this four-drug regimen is used at the beginning of therapy (CDC, unpublished data). Furthermore, a patient who is treated with the four-drug regimen, but who defaults therapy, is more likely to be cured and not relapse when compared with a patient treated for the same length of time with a three-drug regimen.
Picture are showing to you about some of TB case's X-ray

 These chest X-rays show advanced pulmonary tuberculosis. There are multiple light areas (opacities) of varying size that run together (coalesce).
These chest X-rays show advanced pulmonary tuberculosis. There are multiple light areas (opacities) of varying size that run together (coalesce).Arrows indicate the location of cavities within these light areas. The X-ray on the left clearly shows that the opacities are located in the upper area of the lungs toward the back. The appearance is typical for chronic pulmonary tuberculosis but may also occur with chronic pulmonary histiocytosis and chronic pulmonary coccidioidomycosis. Pulmonary tuberculosis is making a comeback with new resistant strains that are difficult to treat. Pulmonary tuberculosis is the most common form of the disease, but other organs can be infected.
Another X-ray on this bellow shows a single lesion (pulmonary nodule) in the upper right lung (seen as a light area on the left side of the picture). The nodule has distinct borders (well-defined) and is uniform in density. Tuberculosis (TB) and other diseases can cause this type of lesion.

Typical signs of tuberculosis are:
- chronic or persistent cough and sputum production. If the disease is at an advanced stage the sputum will contain blood.
- fatigue.
- lack of appetite.
- weight loss.
- fever.
- night sweats.
Tuberculosis can mimic many forms of disease and must always be considered if no firm diagnosis has been made.
Other non-tuberculous mycobacteria found in soil and water can cause disease in susceptible patients with a history of cystic fibrosis, chronic lung damage, alcoholism and immunosuppression (suppression of immune responses by a disease or drugs). These atypical mycobacteria can be present as colonising organisms without necessarily causing disease.
Tuberculosis Treatment
Because administration of a single drug often leads to the development of a bacterial population resistant to that drug, effective regimens for the treatment of TB must contain multiple drugs to which the organisms are susceptible. When two or more drugs are used simultaneously, each helps prevent the emergence of tubercle bacilli resistant to the others. However, when the in vitro susceptibility of a patient's isolate is not known, which is generally the case at the beginning of therapy, selecting two agents to which the patient's isolate is likely to be susceptible can be difficult, and improper selection of drugs may subsequently result in the development of additional drug-resistant organisms.
Hence, tuberculosis is usually treated with four different antimicrobial agents The course of drug therapy usually lasts from 6-9 months. The most commonly used drugs are rifampin (RIF) isoniazid (INH), pyrazinamide (PZA ) and ethambutol (EMB) or streptomycin (SM). When adherence with the regimen is assured, this four-drug regimen is highly effective . Based on the prevalence and characteristics of drug-resistant organisms, at least 95% of patients will receive an adequate regimen (at least two drugs to which their organisms are susceptible) if this four-drug regimen is used at the beginning of therapy (CDC, unpublished data). Furthermore, a patient who is treated with the four-drug regimen, but who defaults therapy, is more likely to be cured and not relapse when compared with a patient treated for the same length of time with a three-drug regimen.
posted by Ocha at
10:48 PM
![]()
![]()








0 Comments:
Post a Comment
Subscribe to Post Comments [Atom]
<< Home